Targeted Probe and Educate Progress Update: DRG 885 - Psychoses
The Centers for Medicare & Medicaid Services (CMS) Change Request 10249 (PDF, 241.88 KB) implemented the Targeted Probe and Educate (TPE) process effective October 1, 2017. The following provides JJ Part A Probe 1 and Probe 2 TPE results statistics from January 2, 2018, to February 28, 2020.
Findings
Medical Review initiated Probe review edits for providers identified through data analysis demonstrating high risk for improper payment. Providers have been offered education throughout and upon completion of the JJ Probe 1 and Probe 2 TPE review. Current JJ Part A Probe 1 and Probe 2 DRG 885 — Psychoses, TPE Results are as follows:
DRG 885 Psychoses
Probes Processed January 2, 2018, to February 28, 2020
| Number of Providers with Edit Effectiveness Performed Probe 1 | Providers Compliant Completed/ Removed After Probe 1 | Providers Non-Compliant Progressing to TPE Probe 2 |
Providers | Number of Providers with Edit Effectiveness Performed Probe 2 | Providers Compliant Completed/ Removed After Probe 2 edit | Providers Non-Compliant Progressing to TPE Probe 3 |
|---|---|---|---|---|---|---|
|
98 |
74 |
24 |
2 |
9 |
9 |
0 |
Findings by State
Palmetto GBA’s overview of results by state for providers who have had edit effectiveness performed for Probe 1 and Probe 2 TPE review from January 2, 2018, to February 28, 2020.
| State | Number of Providers with Edit Effectiveness Performed Probe 1 | Providers Compliant Completed/ Removed After Probe 1 | Providers Non-Compliant Progressing to TPE Probe 2 | Providers Removed for Other Reasons | Number of Providers with Edit Effectiveness Performed Probe 2 | Providers Compliant Completed/ Removed After Probe 2 Edit | Providers Non-Compliant Progressing to TPE Probe 3 |
|---|---|---|---|---|---|---|---|
| Alabama |
30 |
21 |
9 |
0 |
4 |
4 |
0 |
| Georgia |
28 |
22 |
6 |
0 |
2 |
2 |
0 |
| Tennessee |
40 |
31 |
9 |
2 |
3 |
3 |
0 |
| State | Overall Charge Denial Rate Per State Probe 1 | Overall Charge Denial Rate Per State Probe 2 |
|---|---|---|
| Alabama |
17% |
5% |
| Georgia |
16% |
0% |
| Tennessee |
14% |
0% |
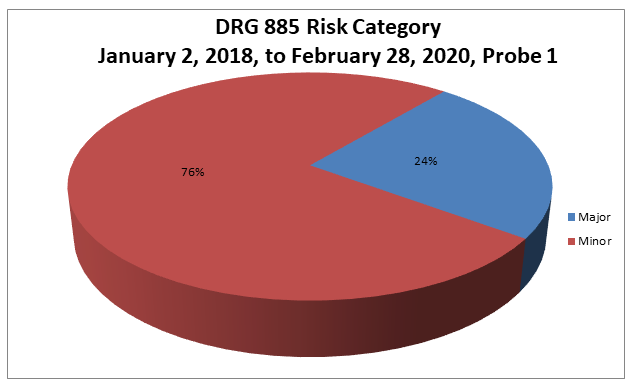
Risk Category
Risk Category is defined based on end of Probe 1 provider error rates. The categories are defined as:
| Risk Category | Error Rate |
|---|---|
|
Minor |
0–20% |
|
Major |
21–100% |
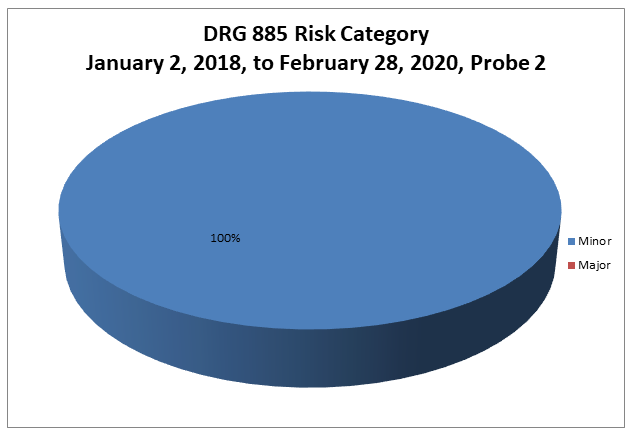
Risk Category
Risk Category is defined based on end of Probe 2 provider error rates. The categories are defined as:
| Risk Category | Error Rate |
|---|---|
|
Minor |
0–20% |
|
Major |
21–100% |
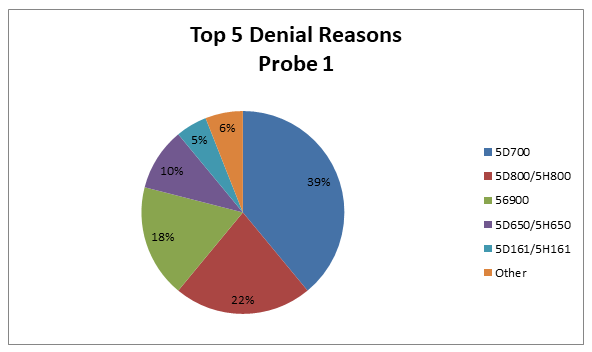
DRG 885
Top 5 Denial Reasons January 2, 2018, to February 28, 2020, Probe 1
- 5D700 — No Valid Plan of Treatment Present
- 5D800/5H800 — Inpatient Psychiatric Services Not Medically Necessary
- 56900 — Auto Deny — Requested Records Not Submitted Timely
- 5D650/5H650 — No Valid Certification/Recertification Present
- 5D161/5H161 — No Physician’s Orders
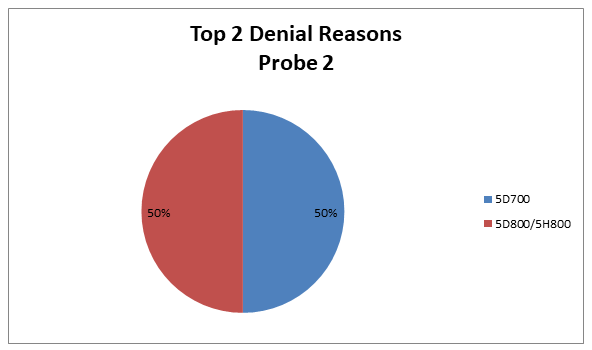
DRG 885
Top 2 Denial Reasons January 2, 2018, to February 28, 2020, Probe 2
- 5D700 — No Valid Plan of Treatment Present
- 5D800/5H800 — Inpatient Psychiatric Services Not Medically Necessary
5D700 — No Valid Plan of Treatment Present
Reason for Denial
The service(s) billed (was/were) not covered because a valid treatment plan established and approved by a physician was not included in the medical records submitted for review as required by Medicare.
How to Avoid a Denial
In order to avoid unnecessary denials for this reason, when responding to an Additional Development Request (ADR), the provider should ensure that the appropriate treatment plan is included and that it is signed by the physician and the mental health professionals contributing to it.
The treatment plan should be developed within the first three days of admission. The focus should be individualized to the patient’s specific strengths and problems as identified in the physician’s psychiatric evaluation, psychosocial and nursing assessments. It should contain a substantiated diagnosis; both short-term and long-range measurable, functional, time-framed goals directed at the individual problems identified as the cause for the patient’s admission; a list of any specific treatment modalities to be utilized in the active treatment of the patient; and a listing of the responsibilities of each member of the treatment team as he/she relates to the plan.
Treatment plan updates should show the treatment plan to be reflective of active treatment, as indicated by documentation of changes in the type, amount, frequency and duration of the treatment services rendered as the patient moves toward expected outcomes. Treatment plan updates should be documented at least weekly, as the physician and treatment team assess the patient’s current clinical status and make necessary changes. Lack of progress and its relationship to active treatment and reasonable expectation of improvement should also be noted.
5D800/5H800 — Inpatient Psychiatric Services Not Medically Necessary
Reason for Denial
Documentation submitted for review did not support the medical necessity for inpatient psychiatric services.
How to Avoid a Denial
In order to avoid denials for this reason, the documentation must provide clear evidence that the acute psychiatric condition being evaluated or treated requires active treatment, including a combination of services such as intensive nursing and medical intervention, psychotherapy, occupational and activity therapy. Patients must require inpatient psychiatric hospitalization services at levels of intensity and frequency exceeding what may be rendered in an outpatient setting, including psychiatric partial hospitalization. There must be evidence of failure at, inability to benefit from, or unacceptable risk in an outpatient treatment setting.
In addition, a complete psychiatric evaluation should be submitted. This evaluation should be completed within 60 hours of the patient’s admission to the psychiatric facility. It should include a medical history, record of mental status; note the onset of the current illness and circumstances leading to admission; describe the behaviors and attitudes of the patient; estimate the intellectual functioning, memory and orientation; provide an inventory of the patient’s assets in a descriptive fashion. In addition to the evaluation, progress notes from all modalities should be submitted in the medical record.
56900 — Auto Deny — Requested Records Not Submitted Timely
Reason for Denial
The services billed were not covered because the medical record(s) was/were not submitted or not submitted timely in response to an Additional Documentation Request (ADR). When an ADR is generated, the provider has 45 days from the date the ADR was generated to respond with medical records. In accordance with CMS instructions, if the documentation needed to make a medical review determination is not received within 45 days from the date of the documentation request, Palmetto GBA will make a medical review determination based on the available medical documentation. If the claim is denied, payment will be denied, or an overpayment will be collected.
How to Avoid a Denial
- Be aware of the ADR date and the need to submit medical records within 45 days of the ADR date
- Submit the medical records as soon as the ADR is received
- Monitor the status of your claims in Direct Data Entry (DDE) and begin gathering the medical records as soon as the claim goes to the status/location of SB6001
- Return the medical records to the address on the ADR. Be sure to include the appropriate mail code or station number. This ensures that your responses are promptly routed to the Medical Review Department.
- Gather all the information needed for the claim and submit it all at one time
- Attach a copy of the ADR request to each individual claim
- If responding to multiple ADRs, separate each response and attach a copy of the ADR to each individual set of medical records. Make sure each set of medical records is bound securely with one staple in the upper left corner or a rubber band to ensure that no documentation is detached or lost. Do not use paper clips.
- Do not mail packages C.O.D.; we cannot accept them
5D650/5H650 — No Valid Certification/Recertification Present
Reason for Denial
The service(s) billed (was/were) not covered because a valid certification/recertification signed by the physician was not included in the medical records submitted for review as required by Medicare.
How to Avoid A Denial
In order to avoid unnecessary denials for this reason, when responding to an Additional Development Request (ADR), the provider should ensure that the appropriate documentation to support certification/recertification is included and that it is signed by the mental health physician.
The initial certification should be completed at the time of admission or as soon thereafter as the patient’s condition reasonably allows. The physician must provide documentation that the services to be furnished on an inpatient basis can reasonably be expected to improve the patient’s condition or are for diagnostic study. There is no particular language or format required for the certification. It may be submitted on provider generated forms, in progress notes, in the records relating to the stay in question; however, it must be signed by the physician. If the certification is delayed it must be submitted with an explanation or other relevant evidence to justify the delay.
Recertification should support that all services provided since the previous certification/recertification were, and continue to be, medically necessary that treatment is expected to improve the patient’s condition or is for diagnostic study. There should be documentation that the patient continues to require active treatment and the supervision of inpatient psychiatric staff daily. The first recertification must be completed as of the twelfth day of hospitalization. Each subsequent certification may be at intervals established by the psychiatric facility on a case-by-case basis. However, the interval is to be no longer than 30 days.
5D161/5H161 — No Physician’s Orders
Reason for Denial
This claim was fully or partially denied because there were no physician’s orders submitted for review for all or some of the services billed.
How to Avoid a Denial
- A physician’s order should be submitted for review with the request for copies of medical records
- A legible signature is required on all documentation necessary to support orders and medical necessity
- The copy of the order should be legible and dated
- Make sure any orders submitted for review are for the date(s) of service billed
Education
Providers are offered an individualized education session where each claim denial will be discussed, and any questions will be answered. Palmetto GBA offers a variety of methods for provider education such as webinar sessions, web-based presentations or teleconferences. Other education methods may also be available.
Next Steps
Providers found to be non-compliant (major risk category/denial rate of 21–100%) at the completion of TPE Probe 1 will advance to Probe 2, and providers found to be non-compliant (major risk category/denial rate of 21–100%) at the completion of TPE Probe 2 will advance to Probe 3 of TPE at least 45 days from completion of the 1:1 post probe education call date. Palmetto GBA offers education at any time for providers. Providers do not have to be identified for TPE to request education.
References
- CMS Targeted Probe and Educate (TPE) web page
- Change Request 10249 (PDF, 241.88 KB)