Targeted Probe and Educate Progress Update: Home Health Progress Update
The Centers for Medicare & Medicaid Services (CMS) Change Request 10249 (PDF, 242 KB) implemented the Targeted Probe & Educate (TPE) process, effective October 1, 2017. The following provides Probe 1 and Probe 2 TPE results statistics from October 1, 2017, to October 2, 2019.
Findings
Medical Review initiated probe review edits for providers identified through data analysis demonstrating high risk for improper payment. Providers have been offered education throughout and upon completion of the Probe 1 and Probe 2 TPE review. Current Probe 1 and Probe 2 Home Health TPE Results are as follows:
Home Health
Probes Processed October 1, 2017 – October 2, 2019
| Number of Providers with Edit Effectiveness Performed Probe 1 | Providers Compliant Completed/Removed After Probe 1 | Providers Non-Compliant Progressing to TPE Probe 2 | Providers Removed for Other Reason | Number of Providers with Edit Effectiveness Performed Probe 2 | Providers Compliant Completed/Removed After Probe 2 | Providers Non-Compliant Progressing to TPE Probe 3 |
|---|---|---|---|---|---|---|
|
1651 |
736 |
913 |
182 |
121 |
69 |
52 |
Findings by State
Palmetto GBA’s overview of results by state, for providers who have had edit effectiveness performed, for Probe 1 and Probe 2 TPE review from October 1, 2017 – October 2, 2019.
| State | Number of Providers with Edit Effectiveness Performed Probe 1 | Providers Compliant Completed/Removed After Probe 1 | Providers Non-Compliant Progressing to TPE Probe 2 | Providers Removed from Probe 1 or 2 for Other Reason | Number of Providers with Edit Effectiveness Performed Probe 2 | Providers Compliant Completed/Removed After Probe 2 | Providers Non-Compliant Progressing to TPE Probe 3 |
|---|---|---|---|---|---|---|---|
| Ala. |
22 |
16 |
6 |
0 |
0 |
0 |
0 |
| Ark. |
16 |
9 |
7 |
2 |
2 |
1 |
1 |
| Fla. |
78 |
43 |
35 |
2 |
0 |
0 |
0 |
| Ga. |
21 |
15 |
6 |
0 |
0 |
0 |
0 |
| Ill. |
N/A |
N/A |
N/A |
N/A |
N/A |
N/A |
N/A |
| Ind. |
34 |
15 |
18 |
4 |
4 |
2 |
2 |
| Ky. |
18 |
11 |
7 |
2 |
2 |
2 |
0 |
| La. |
27 |
15 |
12 |
0 |
0 |
0 |
0 |
| Miss. |
8 |
4 |
4 |
0 |
0 |
0 |
0 |
| N.C. |
29 |
14 |
15 |
0 |
4 |
1 |
3 |
| N.M. |
3 |
1 |
2 |
0 |
1 |
1 |
0 |
| Ohio |
149 |
42 |
107 |
58 |
35 |
13 |
22 |
| Okla. |
52 |
23 |
29 |
0 |
5 |
4 |
1 |
| OT |
13 |
7 |
6 |
1 |
1 |
1 |
0 |
| S.C. |
7 |
1 |
6 |
4 |
0 |
0 |
0 |
| Tenn. |
17 |
9 |
8 |
0 |
1 |
1 |
0 |
| Texas |
1151 |
503 |
648 |
109 |
64 |
42 |
22 |
| ZPIC |
6 |
3 |
3 |
0 |
2 |
1 |
1 |
| State | Overall Charge Denial Rate Per State Probe 1 | Overall Charge Denial Rate Per State Probe 2 |
|---|---|---|
| Ala. |
17.74% |
N/A |
| Ark. |
26.16% |
26.81% |
| Fla. |
25.78% |
N/A |
| Ga. |
18.08% |
N/A |
| Ill. |
N/A |
N/A |
| Ind. |
27.96% |
23.07% |
| Ky. |
19.85% |
17.87% |
| La. |
21.55% |
N/A |
| Miss. |
29.29% |
N/A |
| N.C. |
25.51% |
33.55% |
| N.M. |
34.83% |
0% |
| Ohio |
41.48% |
32.96% |
| Okla. |
28.14% |
12.08% |
| OT |
20.54% |
7.41% |
| S.C. |
37.66% |
N/A |
| Tenn. |
20.34% |
9.24% |
| Texas |
31.66% |
17.24% |
| ZPIC |
25.28% |
19.78% |
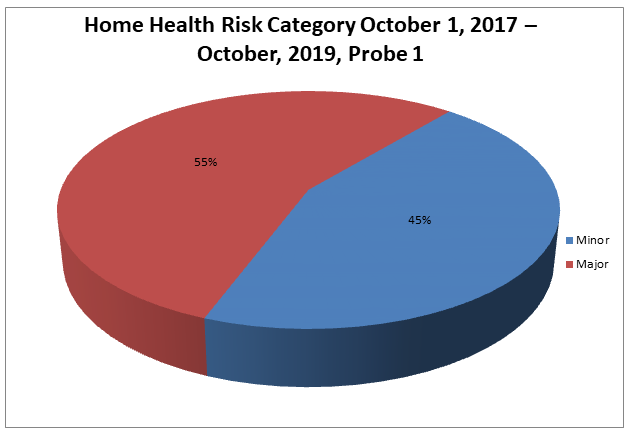
Risk Category
Risk Category is defined based on end of Probe 1 provider error rates. The categories are defined as:
| Risk Category | Error Rate |
|---|---|
|
Minor |
0–20% |
|
Major |
21–100% |
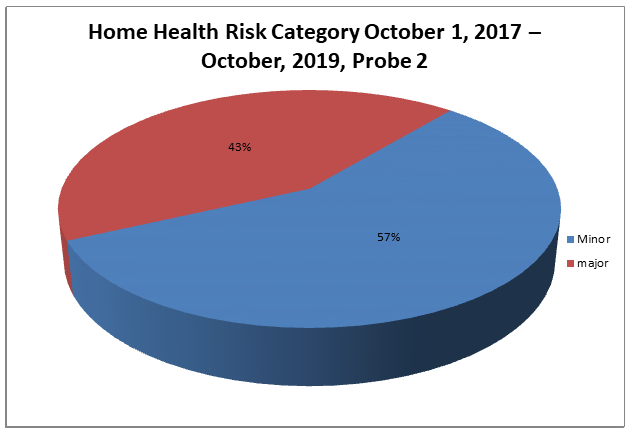
Risk Category
Risk Category is defined based on end of Probe 2 provider error rates. The categories are defined as:
| Risk Category | Error Rate |
|---|---|
|
Minor |
0–20% |
|
Major |
21–100% |
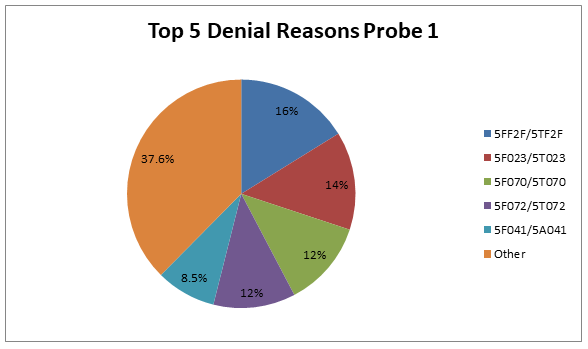
Home Health Probe 1 TPE
Top 5 Denial Reasons October 1, 2017 – October 2, 2019
- 5FF2F/5TF2F — Face-to-Face Encounter Requirements Not Met
- 5F023/5T023 — No Plan of Care or Certification
- 5F070/5T070 — No Documentation of Services Rendered
- 5F072/5T072 — No Physician’s Order for Services or More than Ordered
- 5F041/5A041 — The Documentation Submitted Was Insufficient to Support that the Skilled Nurse Service(s) Billed Was/Were Reasonable and Necessary
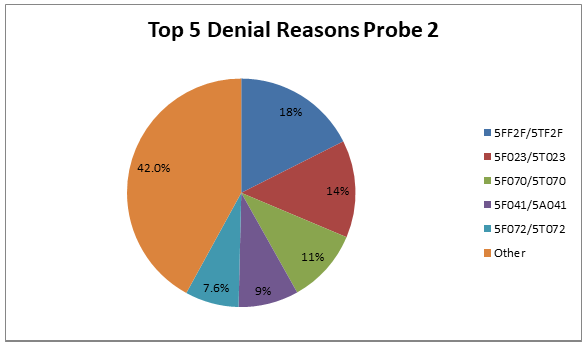
Home Health Probe 2 TPE
Top 5 Denial Reasons October 1, 2017 – October 2, 2019
- 5FF2F/5TF2F — Face-to-Face Encounter Requirements Not Met
- 5F023/5T023 — No Plan of Care or Certification
- 5F070/5T070 — No Documentation of Services Rendered
- 5F041/5A041 — The Documentation Submitted was Insufficient to Support that the Skilled Nurse Service(s) Billed Was/Were Reasonable and Necessary
- 5F072/5T072 — No Physician’s Order for Services or More than Ordered
5FF2F/5TF2F
Reason for Denial
The services billed were not covered because the documentation submitted for review did not include (adequate) documentation of a face-to-face encounter.
How to Avoid a Denial
Specific documentation related to face-to-face encounter requirements must be submitted for review. This includes, but is not limited to, the following:
- A face-to-face encounter must occur no more that 90 days prior to the home health start of care date or within 30 days of the start of the home health care;
- Encounter was related to the primary reason the patient requires home health services; and
- Encounter was performed by a physician or allowed nonphysician practitioner
The certifying physician must also document the date of the face-to-face encounter.
The face-to-face encounter can be performed by:
- The certifying physician;
- The physician who cared for the patient in an acute or post-acute care facility (from which the patient was directly admitted to home health);
- A nurse practitioner or a clinical nurse specialist who is working in collaboration with the certifying physician or the acute/post-acute care physician; or
- A certified nurse midwife or physician assistant under the supervision of the certifying physician or the acute/post-acute care physician
The certifying physician’s and/or the acute/post-acute care facilities medical record for the patient must contain the actual clinical note for the face-to-face encounter visit that demonstrates that the encounter:
- Occurred within the required timeframe;
- Was related to the primary reason the patient requires home health services; and
- Was performed by an allowed provider type
This information can be found most often in, but is not limited to the following examples:
- Discharge Summary
- Progress Note
- Progress Note and Problem List
- Discharge Summary and Comprehensive Assessment
5F023/5T023
Reason for Denial
The services billed were not covered because the home health agency (HHA) did not have the plan of care established and approved by a physician, as required by Medicare, included in the medical records submitted for review and/or the service(s) billed were not covered because the documentation submitted did not include the physician’s signed certification or recertification.
How to Avoid a Denial
- Ensure that the appropriate plan of care (POC) is included and that it is legibly signed and dated by the physician prior to billing
- A plan of care refers to the medical treatment plan established by the treating physician with the assistance of the home health skilled professional. The plan of care contains all pertinent diagnoses; the patient’s mental status, the types of services, supplies, and equipment required; the frequency of visits to be made; prognosis; rehabilitation potential; functional limitations; activities permitted; nutritional requirements; all medications and treatments; safety measures to protect against injury; instructions for timely discharge; or referral and any additional items the HHA or physician chooses to include.
- Ensure that the signed certification or recertification is submitted when responding to an ADR
- The physician must certify that:
- The home health services were required because the individual was confined to his/her home and needs intermittent skilled nursing care, physical therapy and/or speech-language pathology, or continues to need occupational therapy;
- A plan for furnishing such services to the individual has been established and is periodically reviewed by a physician; and
- The services were furnished while the individual was under the care of a physician
- Since the certification is closely associated with the plan of care, the same physician who establishes the plan must also certify to the necessity for home health services. Certifications must be obtained at the time the plan of care is established or as soon thereafter as possible. There is no requirement that a specific form must be used, as long as the intermediary can determine that this requirement is met. When requesting reimbursement for a claim, the provider must have the certification on file and be able to submit this information if medical records are requested by the intermediary.
- The physician must recertify at intervals of at least once every 60 days that there is a continuing need for services and should estimate how long services will be needed. The recertification should be obtained at the time the plan of care is reviewed and must be signed by the same physician who signs the plan of care. When requesting reimbursement for a claim, the provider must have the recertification on file and be able to submit this information if medical records are requested by the intermediary.
5F070/5T070
Reason for Denial
No documentation of services rendered. Documentation of the services(s) billed was not submitted/legible/valid/complete in the medical records submitted in response to the Additional Development Request (ADR). As a result, medical necessity for these services could not be determined.
How to Avoid a Denial
The provider should ensure that adequate documentation is submitted to substantiate the medical necessity for all the services billed when responding to an Additional Development Request (ADR). The provider may submit discipline visit notes and/or a summary of the services rendered for the billing period. If a summary is submitted, it should include the following:
- The information for the dates of service billed;
- Documentation of the services that “were rendered” by each discipline billed;
- Documentation of the patient’s condition; and
- Documentation of the patient’s progress/response to the treatments/services rendered
5F072/5T072
Reason for Denial
Medicare requires that all services be ordered (including discipline, duration, frequency, treatment, legible, signed/dated appropriately) by a physician. The denied visits were not ordered, or exceeded the physician's orders.
How to Avoid a Denial
- When responding to an Additional Development Request (ADR), verify orders for all services rendered and billed are included with the medical records
- Ensure physician orders for all services billed are obtained prior to providing the service and prior to billing the final payment claim to Medicare
5F041/5A041
Reason for Denial
The skilled nursing visit denied were not covered because the documentation submitted in response to the Additional Development Request (ADR) did not support medical necessity for continuation of skilled services.
Initially skilled nursing services were required to observe and assess the beneficiary’s medical condition and response to the plan of care. The key to Medicare coverage is for the documentation to “paint a picture” of the beneficiary’s overall medical condition indicating the need for skilled service.
Skilled observation and assessment beyond a three-week period may be justified when documentation supports the likelihood of further complications or an acute episode. However, observation and assessment are not reasonable and necessary when the documentation indicated that the abnormal findings are part of a longstanding pattern of the patient’s condition and there is no attempt to change the treatment to resolve them.
How to Avoid a Denial
Submit all documentation related to the services rendered and billed to Medicare which supports the medical necessity of the services. Note: A legible signature and date signed is required on all documentation necessary to support orders and medical necessity. Use the most appropriate ICD-10-CM codes to identify the beneficiary’s medical diagnosis/diagnoses.
Submit documentation to support the need for skilled care. Some reasons for services may include, but are not limited to, the following:
- New onset or acute exacerbation of diagnosis (Include documentation to support signs and symptoms and the date of the new onset or acute exacerbation)
- New and/or changed prescription medications — new medications: those the beneficiary has not taken recently, i.e., within the last 30 days. Changed medications: those, which have a change in dosage, frequency, or route of administration within the last 60 days.
- Hospitalizations (include date and reason)
- Acute change in condition (Be specific and include changes in treatment plan as a result of changes in medical condition, e.g., physician contact, medication changes)
- Changes in caregiver status or an unstable caregiving situation (e.g., involvement of many services or community resources, unsafe or unclean environment which interferes with putting the plan into action)
- Complicating factors (i.e., simple wound care on lower extremity for a beneficiary with diabetic peripheral angiopathy)
- Inherent complexity of services; therefore, the services can be safely and effectively provided only by a skilled professional
- Lack of knowledge or understanding of the beneficiary’s care, which requires initial skilled teaching and training of a beneficiary, the beneficiary’s family or caregiver on how to manage the beneficiary’s treatment regime
- Reinforcement of previous teaching when there is a change in the beneficiary’s physical location (i.e., discharged from hospital to home)
- Any type of re-teaching due to a significant change in a procedure, the beneficiary’s medical condition, when the beneficiary’s caregiver is not properly carrying out the task, or other reasons which may require skilled re-teaching and training activities
- The need for a nurse to administer an injection of a self-injectable medication such as insulin or Calcimar. Clinical documentation needs to indicate: (a) the beneficiary’s inability to self-inject and the non-availability of a willing/able caregiver, (b) the appropriate diagnosis to warrant administration of the medication, (c) laboratory results (if required to meet Medicare criteria), and (d) dosage of the medication.
- The need for foley/suprapubic catheter changes and/or assessment/instruction regarding complications
- The need for gastrostomy tube changes and/or assessment/instruction regarding complications
- The need for administration of IM/IV medications based on medical necessity, supporting diagnosis, and accepted standards of medical practice
- Dressing changes for complicated wound care including documentation (at least weekly) of wound location, size, depth, drainage, and complaints of pain
- The need for management and evaluation of a complex care plan. Answering “yes” to the following questions may be helpful in determining this need:
- Is the patient at HIGH RISK for hospitalization or exacerbation of a health problem if the plan of care is not implemented properly (e.g., multiple medical problems or diagnosis, limitations in activities of daily living or mental status, cultural barriers, history of repeated hospitalizations)?
- Does the patient have a complex, unskilled care plan (e.g., many medications, treatments, use of complex or multiple pieces of equipment, unusual use of supplies)?
- Is there an unstable caregiving situation (e.g., involvement of many services or community resources, unsafe or unclean environment that interferes with putting the plan into action)?
- Does it require the skills of a registered nurse or a qualified therapist to ensure safe and appropriate implementation of the plan of care?
Education
Providers are offered an individualized education session where each claim denial will be discussed and any questions will be answered. Palmetto GBA offers a variety of methods for provider education such as webinar sessions, web-based presentations, or teleconferences. Other education methods may also be available.
Next Steps
Providers found to be non-compliant (major risk category/denial rate of 21 to 100 percent) at the completion of TPE Probe 1 will advance to Probe 2, and Providers found to be non-compliant (major risk category/denial rate of 21 to 100 percent) at the completion of TPE Probe 2 will advance to Probe 3 of TPE at least 45 days from completion of the 1:1 post probe education call date. Palmetto GBA offers education at any time for providers. Providers do not have to be identified for TPE to request education.
References